
When my mother's orthopedist first mentioned 'a walker,' I assumed he meant the aluminum frame that every hospital corridor seems to have leaning against a wall. She had just recovered from a hip replacement, she was 79 years old, and she was already nervous about what her mobility would look like going forward. What I did not realize then, and what I wish someone had explained to me in plain terms, is that 'a walker' describes two very different tools with very different safety profiles, fatigue impacts, and long-term outcomes.
The Drive Medical Rollator Walker (ASIN B005S1CHKC, rated 4.6 stars across more than 50,000 reviews) is a four-wheeled rollator with a padded seat, loop brakes, and a storage basket. The standard walker is the classic aluminum frame, typically with two front wheels or rubber tips. Both are covered by insurance in the right circumstances. But they are not interchangeable, and choosing the wrong one for your parent's specific situation can create more fall risk, not less.
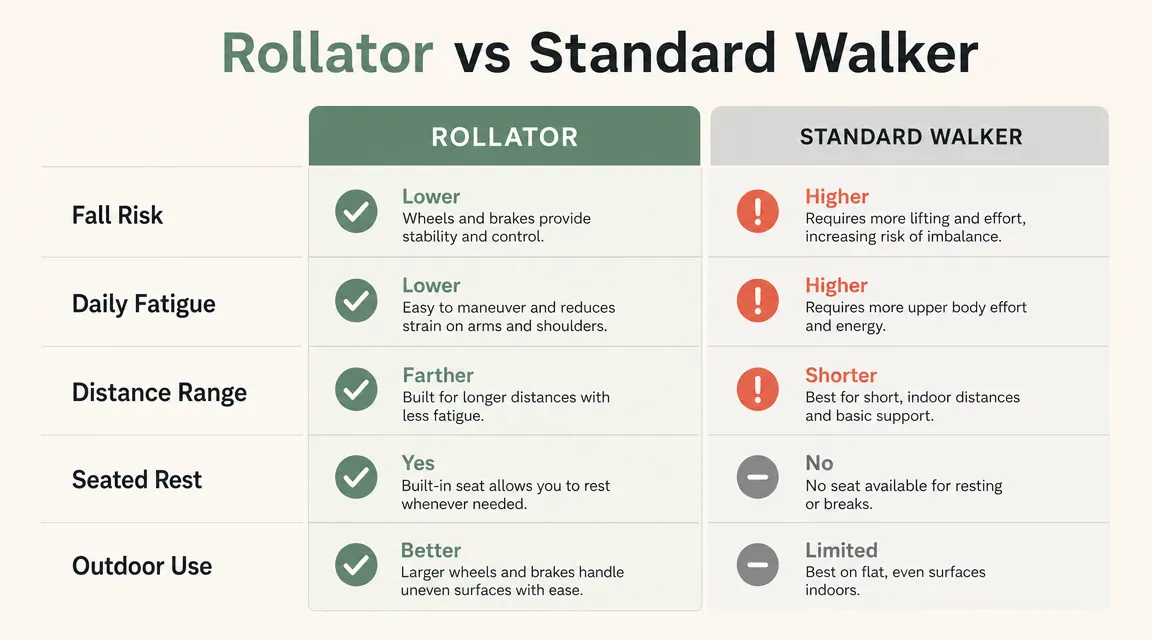
| Feature | Drive Medical Rollator (Left) | Standard Walker (Right) |
|---|---|---|
| Price range | ~$75 on Amazon | $20 to $50 |
| Wheel configuration | Four 6-inch wheels with brakes | Two front wheels or rubber tips |
| Built-in seat | Yes, padded | No |
| Weight supported while moving | Forward lean encouraged, back upright | Full upper-body weight on frame |
| Brake system | Loop brakes, hand-operated | None (friction / tip resistance only) |
| Indoor maneuverability | Good with practice | Excellent |
| Outdoor use on uneven terrain | Good for light outdoor surfaces | Limited |
| Distance capability | Long distances with rest option | Short to moderate distances |
| Fall risk for weak grip | Lower, brakes provide active control | Higher, frame can tip forward |
| Best for | Moderate mobility, long-term independence | Post-surgery stability, very low activity levels |
The short answer: for most seniors who will use their walker more than a few minutes a day, the rollator is the safer long-term choice. The standard walker makes sense in a narrow set of circumstances, which I will describe below. But the default assumption that 'simpler is safer' for older adults is, in my clinical experience, backwards. Simpler often means more fatiguing, which leads to shortcuts, which leads to falls.
If your parent needs a walker that goes the distance without exhausting them, this is where most caregivers land.
The Drive Medical Rollator is the top-selling rollator on Amazon for a reason. Four wheels, padded seat, loop brakes, height adjustable. Ships fast and is available in multiple colors.
Amazon Check Today's Price on Amazon →Where the Rollator Wins
The biggest clinical argument for a rollator is what it does to posture and fatigue over a full day. A standard walker requires the user to lift the frame with every step, place it forward, then bear weight on it. For a senior with arthritis in both hands, reduced grip strength, or any shoulder or wrist involvement, that repetitive lift-place-step pattern is exhausting in a way that most family members do not see until they watch their parent move around for an hour. Fatigue is a direct fall risk. When people tire, they start cutting corners. They shuffle instead of stepping properly. They rush through the lift-and-place sequence. They lean too far forward.
The rollator eliminates that cycle. Because it rolls continuously with the person, there is no lift-and-place. The user walks naturally, keeping the frame moving alongside their gait rather than fighting it. Over a long grocery store trip, a doctor's appointment, or a 30-minute walk around the block, that difference is enormous. My mother told me, about three weeks into using the Drive Medical rollator, that she had forgotten what it felt like to walk without dreading the next hour. That is a clinical outcome worth taking seriously.
The built-in seat is not a luxury. It is a safety feature. Seniors who cannot rest mid-trip push through fatigue because stopping means standing awkwardly or hunting for a chair that may not be there. With a rollator, rest is always one hand-squeeze away. The loop brakes lock the wheels, the user sits on the padded seat, they rest for two minutes, and then they continue. That behavioral change, being willing to rest before they are exhausted rather than after, materially changes fall risk for people who would otherwise push through.
Fatigue is a direct fall risk. When people tire, they start cutting corners. The rollator removes the cycle that creates that fatigue in the first place.

Where the Standard Walker Wins
I want to be honest about when a standard walker is the right call, because there are real situations where it is. Immediately post-surgery, especially after a hip or knee replacement, the surgeon may specifically want limited weight-bearing through a very controlled, deliberate gait. The four-wheeled rollator, precisely because it rolls so easily, can get away from a patient whose coordination and strength are not yet back to baseline. In that narrow window of early recovery, the controlled resistance of a standard walker gives the therapist and the surgeon the ability to monitor exactly how much weight the patient is bearing and through what motions.
A standard walker also makes sense for very small or cluttered living spaces. If your parent's home has narrow hallways, furniture placed close together, or significant rugs and thresholds, the turning radius and rolling momentum of a rollator can feel harder to control than the planted stability of a standard frame. In that case, the better solution is often to combine a rollator for outdoor and longer-distance use with a standard walker or cane for navigating the kitchen and bedroom. It does not have to be one or the other permanently.
The Fall Risk Conversation Nobody Has
In the medical office, I watched providers hand out standard walker prescriptions for years without a conversation about what happens six months later when the patient has adapted to the device but their condition has continued to change. The standard walker gets prescribed at discharge. The patient goes home. They use it for a while. Their grip weakens a bit more, or their balance shifts, or they start going longer distances than the PT ever planned for, and suddenly the device that was right at discharge is not matched to their current functional reality.
The rollator is a better long-term solution because it adapts more gracefully to a wider range of functional levels. As long as a person can use the loop brakes reliably and has enough cognitive awareness to not release the brakes on a slope, the rollator is appropriate across a broad range of mobility levels. I have seen patients in their mid-90s using rollators safely. I have seen 72-year-olds struggle with them because their hands cannot operate the brakes consistently. The device has to match the specific person, not just the diagnosis.
One thing worth asking your parent's physical therapist or physician, if you are not sure which direction to go: 'What does their grip strength look like, and can they reliably squeeze a loop brake?' That single functional question will often settle the rollator-versus-standard decision faster than any feature comparison.
Independence and Dignity: The Factor Nobody Puts on a Spec Sheet
Here is something I have seen over and over, both in the office and with my own mother. When an older adult feels like their mobility device is limiting them, they use it less. And when they use it less, they are less safe. A standard walker, particularly one without a seat, signals to the user that they can only go so far, that there is no backup plan if they get tired, that every outing requires someone else nearby. That anxiety is not imaginary, and it changes behavior in ways that compound over time.
My mother went from barely leaving the house to making her own grocery run within two months of switching to the rollator. She did not ask me to come. She just went. That kind of independence, not dramatic, just ordinary errand-running, is what keeps older adults physically active, socially connected, and cognitively engaged. A device that supports that outcome is not a luxury upgrade. It is a health intervention.

Who Should Buy the Rollator
The Drive Medical Rollator is the right choice for a senior who walks more than 10 to 15 minutes at a stretch, goes outdoors regularly, has any arthritis or grip weakness that makes the lift-and-place pattern tiring, benefits psychologically from knowing they can sit down at any point, or has the cognitive ability to operate loop brakes consistently. That describes the majority of people in their 70s and 80s who need a walker. It is not a device for people who are severely cognitively impaired or who lack the hand strength to operate the brakes safely, but for the broad middle of the population that walkers are designed for, this is a significantly better solution than the standard frame.
Who Should Skip the Rollator
Skip the rollator, at least temporarily, if your parent is in the immediate post-surgical phase and their PT or surgeon has specifically recommended a standard walker or front-wheeled walker for the recovery window. Also skip it if your parent cannot reliably squeeze and hold the loop brakes, lives in a very small apartment with tight corners and multiple thresholds, or has moderate-to-severe cognitive impairment that makes a rolling device unsafe. In those cases, a standard walker, a quad cane, or a different mobility aid may be the right call. This is a situation where getting one PT evaluation, even a one-time consult, is worth the time.
The rollator that 50,000 caregivers trusted is still the one I would recommend today.
The Drive Medical Rollator Walker ships quickly, assembles without tools, and comes in a range of colors. Height adjustable, padded seat, storage basket, loop brakes. Check the current price on Amazon before your parent's next appointment.
Amazon Check Today's Price on Amazon →